
Physiology Friday #292: Does Extreme Exercise Elevate Heart Disease Risk?
A review of the literature, brought to you by Consensus.


Greetings!
Welcome to the Physiology Friday newsletter.
Most of my waking hours are spent searching for and reading the latest scientific research. Given the sheer volume of it, this is no easy task.
Artificial intelligence has been an indispensable tool in this regard. I can collect, summarize, and analyze research in ways I never could before as a one-man team. With one or two queries, I can find answers to any scientific question imaginable. It’s like having a personal research assistant.
But AI has also become a (sometimes unreliable) crutch. It makes it easy to generate quick content for clicks—content which (when not accurately double checked) may contain errors or complete hallucinations of data or references. One must be prudent in their own analysis of the quality of the research AI gives them.
As a researcher, I’m learning how to responsibly embrace the tools AI gives us. And the best tool I’ve found for this job is Consensus, an AI-powered academic search engine built on a database of over 220 million (and counting!) peer-reviewed research papers. Unlike general AI tools, every response is tied back to a real research paper and is grounded in scientific research. It helps you quickly review the literature and understand complex topics faster—all by typing one simple question into the search bar. You don’t need to be an academic to use it either.
I use Consensus every single day. Seriously. And today, I wanted to show you how Consensus works by generating a literature review of one of my favorite topics—extreme endurance exercise and heart disease risk.
For this post, I used Consensus’ Deep Research feature to generate a literature review of 50 papers on one specific topic.
If you’re impressed with Consensus and want to try it out, they’re giving my audience 1 month of Consensus Pro for FREE. Just use this link.

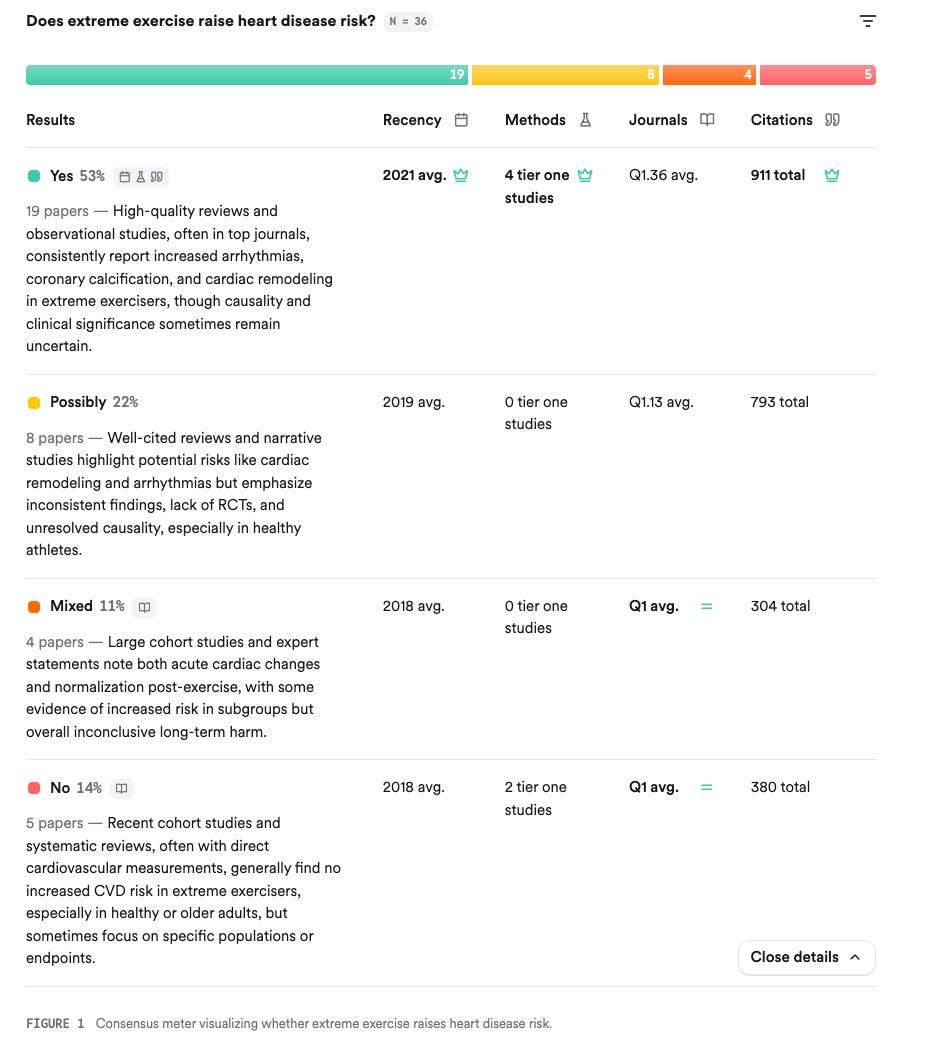
Query: Does extreme exercise raise heart disease risk?
No, most evidence suggests extreme exercise does not raise overall heart disease risk in healthy individuals, but it may increase the risk of specific cardiac conditions (like atrial fibrillation, coronary artery calcification, and myocardial fibrosis) in some subgroups.
1. Introduction
The relationship between extreme exercise and heart disease risk has been the subject of considerable debate. While regular moderate-to-vigorous physical activity is well established as cardioprotective, recent research has explored whether very high volumes or intensities of exercise—such as those performed by endurance athletes—could paradoxically increase the risk of certain cardiovascular conditions. The majority of studies indicate that extreme exercise does not increase overall heart disease risk or mortality in healthy individuals, and elite athletes often have greater longevity than the general population. However, there is accumulating evidence that extreme, long-term endurance exercise may be associated with a higher prevalence of specific cardiac abnormalities, including atrial fibrillation, coronary artery calcification, myocardial fibrosis, and, in rare cases, sudden cardiac death—especially in those with underlying or unrecognized heart disease.
The clinical significance of these findings remains uncertain, and the absolute risk for most individuals remains low. This review synthesizes the current evidence on the potential risks and benefits of extreme exercise for cardiovascular health.
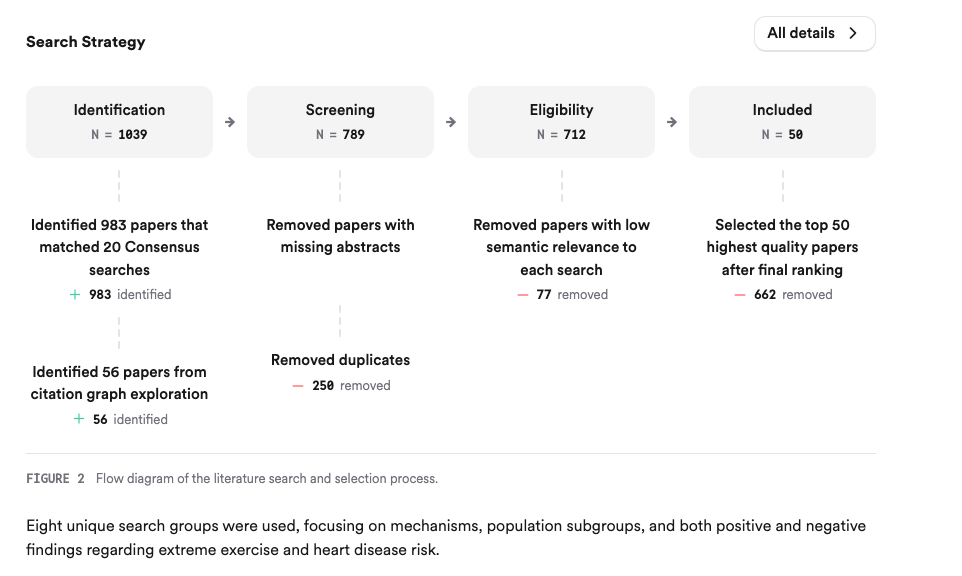
2. Methods
A comprehensive literature search was conducted across over 170 million research papers in Consensus, including sources such as Semantic Scholar and PubMed. The search strategy targeted foundational theories, mechanisms, population studies, and consensus statements on extreme exercise and cardiovascular risk. In total, 1,039 papers were identified, 789 were screened, 712 were deemed eligible, and the 50 most relevant and high-quality papers were included in this review.
3. Results
3.1. Overall Cardiovascular Risk and Mortality
Most large-scale epidemiological studies and consensus statements confirm that regular physical activity, even at high volumes, is associated with reduced cardiovascular morbidity and mortality. Elite endurance athletes generally live longer than the general population. However, some studies suggest a U-shaped or reverse J-shaped relationship, where the benefits of exercise may plateau or slightly decline at the highest levels of activity, particularly in those with pre-existing heart conditions.
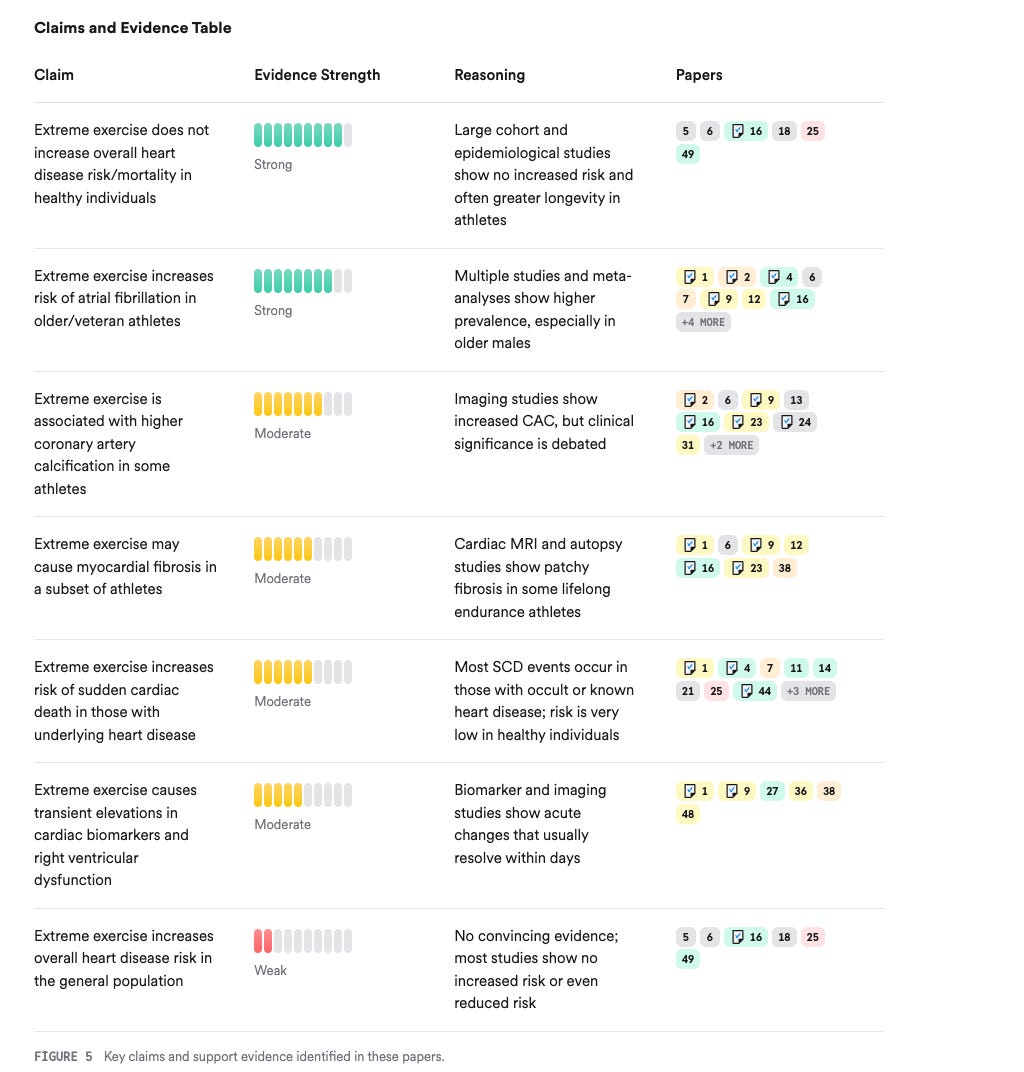
3.2. Specific Cardiac Abnormalities in Extreme Exercisers
Evidence indicates that extreme endurance exercise may increase the risk of certain cardiac conditions:
Atrial fibrillation: Higher prevalence in veteran endurance athletes, especially older males.
Coronary artery calcification (CAC): Some studies report increased CAC in high-volume exercisers, but the clinical significance is debated, as these plaques may be more stable.
Myocardial fibrosis: Patchy fibrosis has been observed in some lifelong endurance athletes, potentially predisposing to arrhythmias.
Arrhythmias and sudden cardiac death: The absolute risk is very low, but extreme exercise can trigger events in susceptible individuals, particularly those with underlying structural or genetic heart disease.
3.3. Mechanisms and Biomarkers
Extreme exercise can cause transient elevations in cardiac biomarkers (troponins, BNP), acute right ventricular dysfunction, and increased sympathetic activity, but these changes usually resolve within days and are not clearly linked to long-term harm in most individuals. Chronic, repetitive stress may contribute to structural changes in a subset of athletes.
3.4. Population Subgroups and Modifying Factors
Risks may be higher in:
Older athletes and those with pre-existing or occult heart disease.
Individuals with genetic predispositions (e.g., arrhythmogenic cardiomyopathy).
Males appear more susceptible to some adverse remodeling effects than females.
4. Discussion
The preponderance of evidence supports the notion that extreme exercise does not increase overall heart disease risk or mortality in healthy individuals, and the benefits of physical activity far outweigh the risks for most people. However, there is credible evidence that extreme, long-term endurance exercise may increase the risk of specific cardiac conditions, such as atrial fibrillation, coronary artery calcification, and myocardial fibrosis, particularly in older male athletes and those with underlying heart disease. The clinical significance of these findings is still being debated, as many of these abnormalities may not translate into increased clinical events or mortality.
The mechanisms underlying these risks include repetitive hemodynamic stress, transient right ventricular dysfunction, and possible cumulative myocardial injury. Genetic predisposition and other individual factors play a significant role in determining risk. Importantly, the absolute risk of adverse events remains very low, and the vast majority of individuals benefit from regular exercise.
5. Conclusion
In summary, extreme exercise does not appear to raise overall heart disease risk in healthy individuals and is associated with increased longevity. However, it may increase the risk of specific cardiac conditions—such as atrial fibrillation, coronary artery calcification, and myocardial fibrosis—in certain subgroups, particularly older male athletes and those with underlying heart disease. The absolute risk remains low, and the benefits of regular physical activity far outweigh the potential risks for most people.
5.1. Research Gaps
Despite extensive research, important gaps remain regarding the long-term clinical significance of cardiac abnormalities observed in extreme exercisers, the mechanisms underlying these changes, and the identification of individuals at greatest risk.
5.2. Open Research Questions
Future research should focus on clarifying the clinical significance of cardiac abnormalities in extreme exercisers, identifying at-risk individuals, and developing evidence-based guidelines for safe exercise at high volumes.
In conclusion, while extreme exercise may increase the risk of certain cardiac conditions in specific populations, it does not raise overall heart disease risk in healthy individuals, and the benefits of regular physical activity remain overwhelming.
Thanks for reading. See you next Friday.
~Brady~

The VO2 Max Essentials eBook is your comprehensive guide to aerobic fitness, how to improve it, and its importance for health, performance, and longevity. Get your copy today and use code SUBSTACK20 at checkout for a 20% discount. You can also grab the Kindle eBook, paperback, or hardcover version on Amazon.

Ketone-IQ is high-performance energy in a bottle. I use it for post-exercise recovery along with enhancing focus, mood, and cognition. Take 30% off your order.

Create is the first “modern creatine” brand. They sell a wide range of creatine monohydrate gummies—and yeah, their gummies actually contain creatine, unlike some other brands. They’re giving my audience 20% off their order. So stock up!
very interesting, and timely! (just found your Stack, based on the story below)
I'm 70 yo male, lotta running miles over last 30 years (+40 marathons). Been prediabetic for all these years (a1C 5.9 - 6.5).
Earlier this year, based on CGM use, determined/eliminated grains and processed carbs, etc). Latest lipid results much improved (i.e., triglycerides go from 150 to 60, HDL go from 40's to 62, 35d...). LDL still a little high (149) and a1C now 6.1. All other stats are good to excellent.
New Dr suggested CAC. Results come back:
Agatston score: The total (aggregate) calcium score utilizing the AJ–130 method is 977. Total volume score is 810.
This means that 10% of similar patients will have a higher calcium score.
Individual major vessel AJ–130 scores are:
LMA: 57, volume score 47
LAD: 835, volume score 678
LCx: 0
RCA: 85, volume score 85
Other: 0
Other findings: Heart and great vessels are normal in size. No pericardial or pleural effusion. Visualized lung fields are clear.
To my uneducated, curious nerd runner's assessment, this don't look so good!!!
Doc appointment is in 2 weeks. Assume if this were imminent death, he'd call me and tell me to go straight to OR!!!
But the running addict that I am, I've kept up my 20 mile/week and feel great!! Next marathon planned for May 2026!
Looking forward to my Dr's assessment and recommendations!
My beef with these studies is the definition of "extreme," or consistent lack thereof.
I've run more than 130,000 miles in the previous 46 years. Sounds extreme!
Or maybe not--it basically works out to averaging a little more than an hour a day during that time, with probably something like 85% of that at an easy to medium intensity. Sounds moderate!
Other would-be definers, such as number of marathons run, are also unhelpful. Is a marathon running 26.21 miles as fast as possible on the day? Covering that distance at a jog? There's no consistency in what people mean by that.