
Why VO₂ Max Still Matters
Is it still a biomarker of health and longevity?


VO2 max is probably one of the topics I’ve written about most. And hopefully, I’ve not beaten a dead horse here. I just think there’s endless interest in it, and I don’t think it’s the “fad” people make it out to be.
Even though the importance of VO2 max has been underscored by myself and others on numerous occasions, VO2 max has made its way back into the mainstream conversation for a different reason—people are questioning its validity as a true “longevity biomarker.” Because of that, I felt like it would be nice to provide a “state-of-the-science” update.
I’ve been doing the podcast rounds lately, and it has allowed me to brush up on the research regarding VO2 max as a longevity biomarker. That’s what this post is about, plus the most up-to-date research on how to improve it with training and other tactics. If you want a somewhat deeper dive into the science, you can pick up my book “VO2 Max Essentials” on Amazon.
Why VO2 max still matters
VO2 max remains one of the most discussed metrics in exercise physiology, and for good reason. It is the maximal rate at which the body can take up, transport, and utilize oxygen during intense exercise, and it is widely regarded as the gold-standard laboratory measure of cardiorespiratory fitness (CRF). The American Heart Association reinforced the clinical importance of CRF in their latest update, arguing that it should be routinely assessed in healthcare and even framing it as a clinical vital sign.1
That said, VO2 max is often discussed too loosely. It is not a standalone “longevity score,” and it is not interchangeable with every estimate of aerobic fitness produced by a treadmill test, population equation, or (especially) wearable. It is a specific physiological construct that we should interpret with nuance.
What VO2 max actually reflects
Physiologically, VO2 max is best understood as an integrative property of the oxygen transport system. It depends on pulmonary gas exchange, cardiac output, blood oxygen carrying capacity, distribution of blood flow, and the ability of working muscles to extract and use oxygen. It reflects how well the body can deliver and utilize oxygen when the demand for aerobic energy production is at its highest (e.g., during maximal exercise).
That systems-level nature is what, in my opinion, makes VO2 max so compelling.
It is not simply a marker of “cardio” in the casual sense. It is a summary readout of how multiple organ systems perform together under stress. At the same time, it does not fully determine endurance performance on its own. Endurance outcomes also depend heavily on economy, durability, and the fraction of VO2 max that can be sustained near threshold, hence why the guy or girl with the highest VO2 max doesn’t always win the race.
Where the longevity evidence is strongest
There’s no question that a higher level of fitness is associated with a lower risk of dying.
A 2024 overview of meta-analyses2 synthesized 26 systematic reviews representing 199 unique cohort studies and more than 20.9 million observations.
Across those data, higher CRF was strongly and consistently associated with lower all-cause mortality, lower cardiovascular mortality, and lower risk of several chronic disease outcomes.
High versus low CRF was associated with a 53% reduction in all-cause mortality risk, and each 1 metabolic equivalent (1-MET, equal to 3.5 ml/kg/min of oxygen uptake) was associated with an 11% to 17% lower risk of all-cause mortality depending on the meta-analysis.
Those are impressive associations, but the certainty should not be overstated. The same overview rated the certainty of evidence across outcomes from very low to moderate. That does not weaken the overall signal, which is clearly strong and consistent, but it does argue for some caution when translating these epidemiologic associations into sweeping mechanistic claims. And I should note that many studies here were not actually about directly measured VO2 max. They are about CRF more broadly. So let’s discuss that…
VO2 max and CRF are related, but they are not interchangeable
A recent source of controversy is not whether aerobic fitness is important, but whether VO2 max is a useful, meaningful marker worth measuring (separately from CRF, that is).
This arose because many of the most cited mortality studies do not rely on direct breath-by-breath laboratory measurement of VO2 max. Instead, they often use objectively measured exercise capacity expressed in METs, treadmill-estimated CRF, or even non-exercise CRF estimation models.
How much does that matter? Maybe not a lot if we’re talking strength of associations.
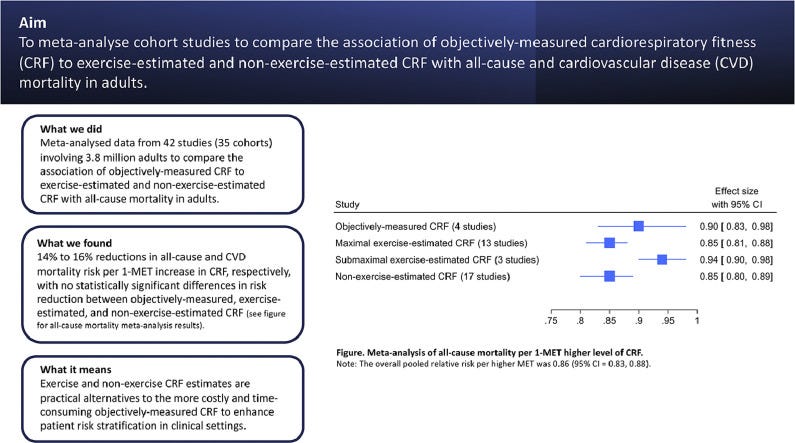
A 2025 systematic review and meta-analysis3 of 42 studies representing 35 cohorts and 3.8 million observations found:
Objectively measured and estimated CRF showed broadly similar dose-response associations with all-cause and cardiovascular mortality.
Per 1-MET higher CRF, all-cause and cardiovascular mortality dropped by 14% and 16%, respectively, without statistically significant differences between objective and estimated approaches.
That is important because it supports the broader conclusion that fitness is a powerful risk marker, regardless of how it’s measured. Nevertheless, the epidemiology is strongest for CRF as a construct. VO2 max is the gold-standard laboratory expression of that construct, but the two are not perfectly synonymous in the literature. I’m willing to accept that, but I’m not quite convinced the semantics matter if we’re talking about longevity in the general sense.
Is VO2 max a biomarker?
Whether VO2 max should be called a biomarker depends largely on how the term is being used. If the intended meaning is an objective, reproducible measure associated with future health outcomes, then VO2 max or CRF clearly behaves like one.
If the intended meaning is a singular mechanistic readout of biological aging, the label becomes much harder to defend. The American Heart Association’s framing is more conservative and more useful: CRF is a vital sign because it provides meaningful prognostic information that improves risk assessment and clinical management. That is, it tells you more about your health when paired with common cardiovascular disease biomarkers (and probably more on its own than any single risk factor like cholesterol, blood glucose, or whether or not you smoke).
I think the most defensible description is that VO2 max is an integrative functional marker. It compresses a great deal of physiology into one number, but it does not function like a magic molecular biomarker that fully explains why one person lives longer or ages better than another.
