
Physiology Friday #278: Do Post-Exercise Levels of Cardiac Damage Predict Heart Disease in Endurance Athletes?
The evolving story on exercise and atherosclerosis.

Greetings!
Welcome to the Physiology Friday newsletter.
I’m running a Prime Day sale on premium subscriptions to Physiologically Speaking. Today only, you can claim 30% off of a monthly or annual subscription. A subscription gets you access to all of my subscriber-only articles plus the entire archive of newsletters, deep dives, videos, and more! Claim the deal below.
Details about the other sponsors of this newsletter, including Ketone-IQ, Examine.com, and my book “VO2 Max Essentials,” can be found at the end of the post. You can find more products I’m affiliated with on my website.
Can you exercise too much?
If there’s one topic I’ll keep returning to every time a new study comes out, it’s endurance exercise and heart disease. This isn’t just because of my personal investment as a lifelong endurance athlete—it’s also because the science is intriguingly complex and continually evolving.
At first glance, the relationship between endurance exercise and heart disease seems paradoxical. After all, exercise is supposed to protect the heart, right? Yet, research consistently shows that athletes who engage in high levels of endurance activity over a lifetime, often known as masters athletes, can have surprisingly high rates of coronary artery calcium—a marker of subclinical atherosclerosis and heart disease. While many of these studies involve small cohorts and potential confounding factors (like participants who adopted endurance sports later in life after years of unhealthy habits like smoking), the pattern still raises important questions.
One theory suggests endurance exercise, when done in very high amounts, might cause acute and chronic cardiac damage, eventually promoting heart disease. But accurately predicting who might develop heart disease and why remains elusive.
A key marker for cardiac stress or damage is cardiac troponin, which increases after events like heart attacks but also after intense endurance efforts such as marathons. Post-exercise troponin elevations were once considered to be harmless because they were relatively common, healthy athletes experienced them, and they occurred without apparent symptoms (and eventually resolved). However, studies have shown that people with abnormally high levels of troponin after exercise are at an elevated risk of cardiovascular events and even death. In other words, post-exercise troponin may be a sign of future risk and not a benign outcome.
What’s not clear is whether athletes with existing heart disease or significant coronary artery calcium show exaggerated troponin responses compared to healthy athletes. If so, this could reveal underlying cardiac disease in otherwise asymptomatic athletes.
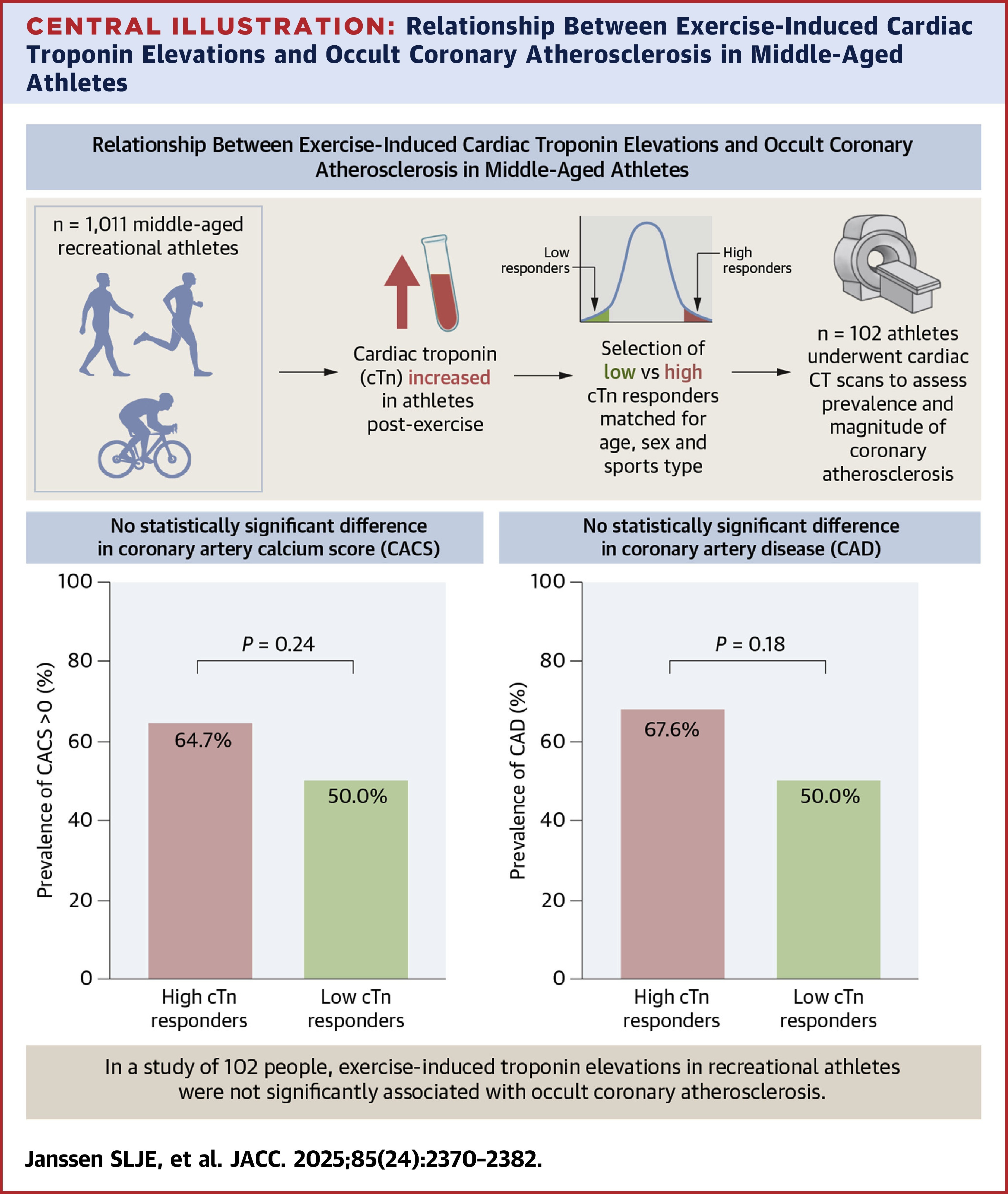
Thanks to new research, we now have clearer insights into this critical question.1

For the study, researchers gathered a group of recreational athletes who were participating in walking, cycling, and running events, measuring pre-exercise and post-exercise levels of high-sensitivity cardiac troponin T (hs-CTnT) and troponin I (hs-cTnI)—markers of cardiac injury
The sample included 497 walkers, 122 cyclists, and 398 runners with an average age of 56 (62.7% of them were men).
They then took people with the highest levels of post-exercise troponin and the lowest levels (“high responders” and “low responders”, respectively corresponding to 10% of the total study sample with 68 high responders and 34 low responders) and performed scans of their heart (a cardiac CT scan) within 3 months of completing the respective endurance exercise events. These scans were used to obtain a coronary artery calcium score (CAC score), degree of artery narrowing (stenosis), and plaque types (calcified, partially calcified, or non-calcified) for each participant.
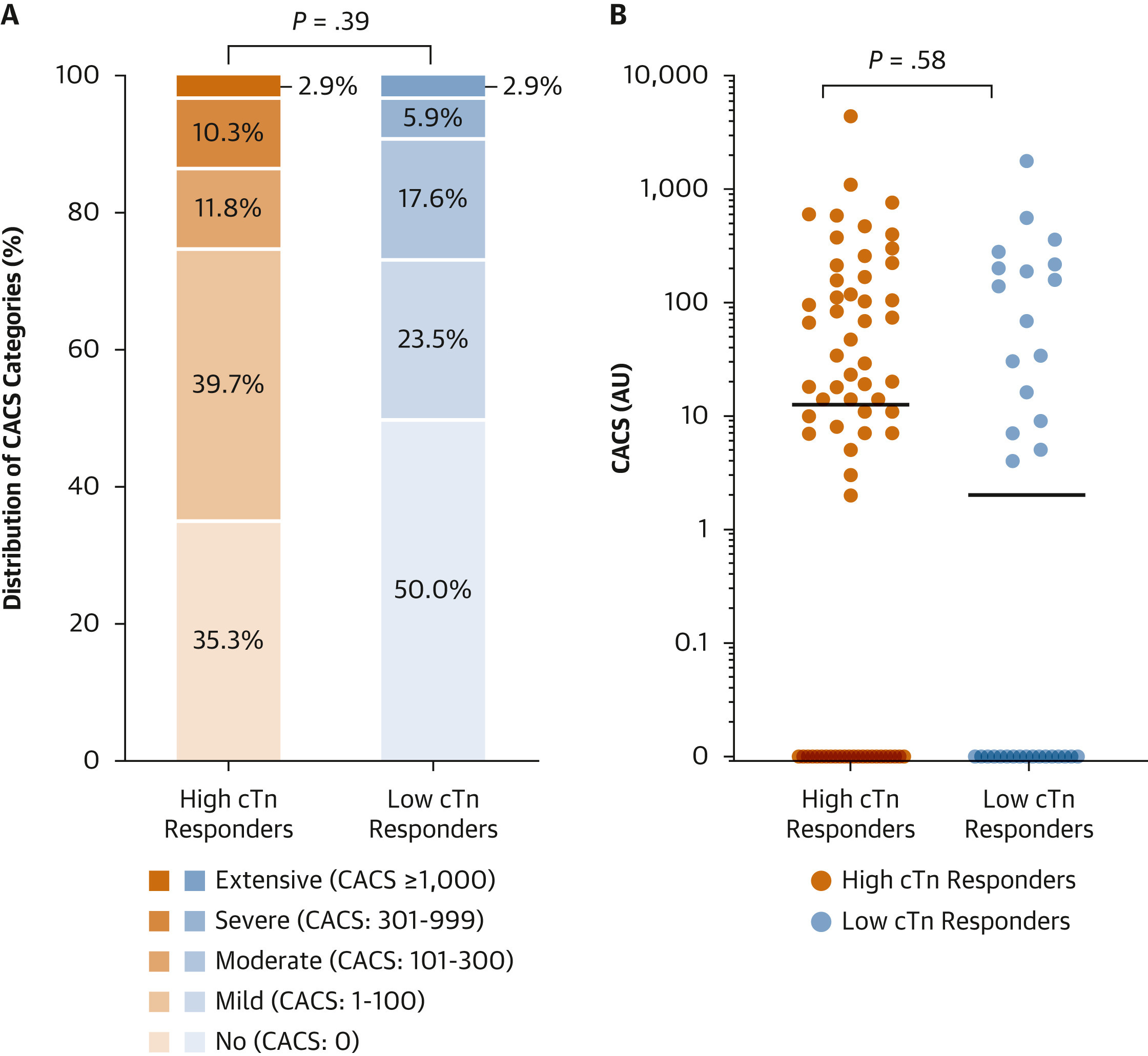
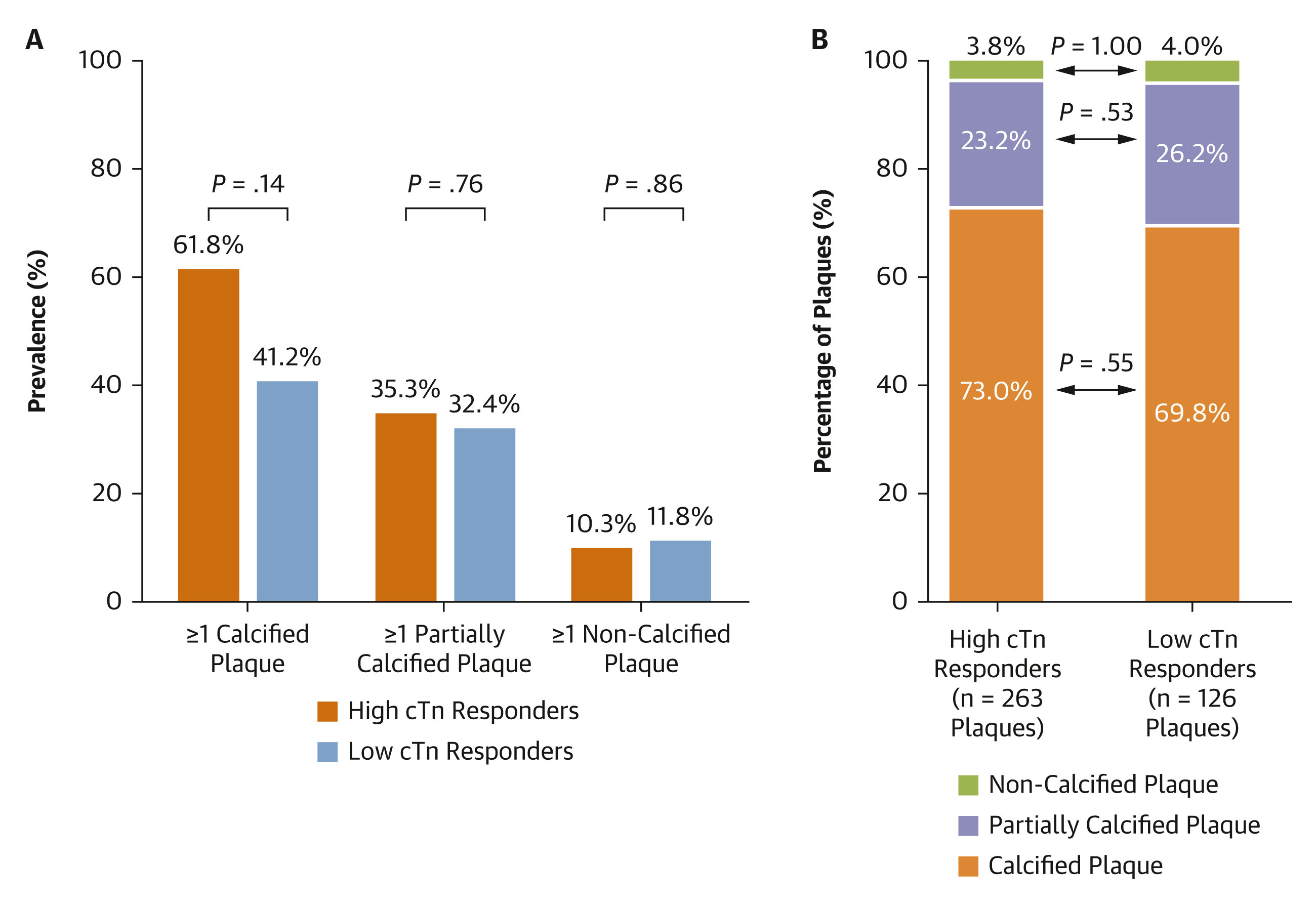
CAC scores weren’t different between the high-responders and low-responders, and despite 61/102 athletes having a CAC score above 0 (indicative of heart disease), the prevalence of athletes with a score above zero wasn’t different among the high responders (65%) and low responders (50%). These findings extended to plaque burden—the distribution of calcified, partially calcified, and non-calcified plaques was similar between high and low responders. Interestingly, among all of the athletes, calcified plaques were most common, followed by partially and non-calcified plaques—that’s a finding that agrees with previous literature
What about the relationship between post-exercise increases in troponin and CAC scores? It turns out, there is none. While resting levels of hs-cTnT were correlated with CAC scores, post-exercise levels and the pre- to post-exercise change of both hs-cTnT and hs-cTnI were not—athletes with larger changes in post-exercise troponin did not have apparently higher levels of heart disease.
There was one association that was marginally significant: greater post-exercise hs-cTnT and larger pre- to post-exercise changes in both hs-cTnT and hs-cTnI were associated with a higher CAD-RADS classification, a score that ranges from 0–5 that indicates the severity of coronary artery stenosis or occlusion (5 being the highest score indicative of total occlusion)
Though the study’s results failed to support the authors’ hypotheses, we can still learn a lot from the findings.
What’s noteworthy is the number of athletes who had post-exercise troponin levels above the upper reference limit—nearly 52% for hs-cTnT and 16% for hs-cTnI. This tells us that, among recreational athletes, exercise appears to produce a nearly ubiquitous rise in cardiac injury biomarkers that veer into the “looks like a heart attack” category.
Furthermore, coronary artery disease is relatively common among recreational athletes; atherosclerosis was present among 62% of this highly-active study population. That also agrees with numbers reported in the literature on masters athletes (~60–70% of whom have detectable levels of atherosclerosis).
The novel finding of this study, then, is that these two phenomena aren’t related—rises in cardiac injury biomarkers after exercise don’t seem to predict who does or doesn’t have coronary artery disease.
To quote the authors: “The majority of the inter-individual variation in the magnitude of the exercise-induced cTn elevations in recreational athletes is not attributable to occult coronary artery disease [but rather] unknown factors.”
Should we be surprised, or perhaps even worried, about the high(ish) rates of heart disease in this cohort and the fact that a lot of them experienced large spikes in troponin after exercise? After all, many of us probably resemble these “recreational athletes” both demographically and in our exercise habits.
Honestly, I’m not sure. The reported exercise intensity of the activities the participants engaged in prior to their post-exercise troponin measurements was fairly high—around 80% of age-predicted maximal heart rate for the walkers and cyclists and 95% for the runners. That could potentially explain why cardiac injury biomarkers were somewhat high. The magnitude of post-exercise troponin does depend somewhat on exercise intensity and duration.
What I think we should take away from this study is that there still isn’t a cut-and-dried answer to “does endurance exercise cause heart disease?” Some people who run (or walk or ride) a lot will develop heart disease. Some people who don’t run (or walk or ride) at all will develop heart disease. And the people who run (or walk or ride) the most won’t always develop heart disease at a higher rate than those who engage in these activities less.
Is endurance exercise risky? Sure it is. But right now, we still don’t have accurate ways to predict who it might be most risky for, at least when it comes to heart disease.
Until we do, the best thing any of us can do is practice diligence with our diet and stress levels, consider our family history, and be sensible about how much (and how hard) we exercise.
I’m still working on that last one…
Thanks for reading. See you next Friday.
~Brady~

The VO2 Max Essentials eBook is your comprehensive guide to aerobic fitness, how to improve it, and its importance for health, performance, and longevity. Get your copy today and use code SUBSTACK20 at checkout for a 20% discount. You can also grab the Kindle eBook, paperback, or hardcover version on Amazon.

Examine.com: Examine is the largest database of nutrition and supplement information on the internet.

Ketone-IQ is high-performance energy in a bottle. I use it for post-exercise recovery along with enhancing focus, mood, and cognition. Take 30% off of your order.
Important to say that the list of conditions associated with elevated troponin is long. Similar studies have shown that patients commonly have elevated troponin after non-cardiac surgery, for example. These patients also probably have a worse long term prognosis. But it’s not clear what and how to intervene to improve their chances. Also, troponin is eliminated from the body by the kidney and mild, transient kidney failure is common after endurance exercise. Potentially confounding these results.
I believe diet has more to do with plaque buildup in the arteries and over a lifetime endurance athletes may not have better diets however I didn't take from the article that endurance athletes have higher rates of heart disease than the general public.