
Physiology Friday #307: Should Exercise Guidelines Be Personalized?
Cardiovascular risk should be part of the equation when considering how much activity someone does (and how hard it should be).


Greetings!
Welcome to the Physiology Friday newsletter.
Details about the sponsors of this newsletter and deals on products I love, including Ketone-IQ, Create creatine, Equip Foods, and ProBio Nutrition can be found at the end of the post.
The physical activity guidelines are good. But like most public health recommendations, they’re not perfect.
Part of that imperfection (or at least their real-world ineffectiveness) probably has nothing to do with the guidelines themselves, and everything to do with the fact that most people don’t follow them. Only around 25% of adults in the United States meet the weekly physical activity guidelines for aerobic and strength training.1
So yes, one could argue this reflects a human limitation more than a guideline problem.
But there’s a deeper issue. As I’ve discussed in a prior newsletter—and even talked about with Dr. Rhonda Patrick on her podcast—the guidelines rely on a somewhat anachronistic way of equating exercise intensity. They assume that one minute of vigorous exercise is “worth” two minutes of moderate exercise. That equivalence makes sense for calorie burn. But when it comes to health outcomes and chronic disease risk, vigorous activity’s benefits often look disproportionately (even exponentially) larger than those of light- or moderate-intensity activity.
That brings up another limitation of the guidelines, one that’s especially relevant for disease prevention. They largely assume that everyone, regardless of health status or disease risk, will benefit from the same basic target of 150 to 300 minutes of activity per week (or 75 to 150 minutes if that activity is more intense). In other words, they’re essentially one-size-fits-all recommendations (which, in some ways, feels a bit like an exercise version of the Dietary Guidelines for Americans… which I have some thoughts on).
The problem is that physiology is about as far from one-size-fits-all as it gets. Genetics, environment, and lifestyle constraints all shape what someone can do (and what they should do), especially when the goal is reducing disease risk.
That’s why this new study caught my attention.2 It tried to tackle the idea of personalized physical activity prescriptions for reducing cardiovascular disease risk, based on a person’s predisposition, or baseline risk, for developing cardiovascular disease. The authors even put some specific numbers and thresholds on total activity, duration, and intensity, which is helpful. But what stood out to me even more was the broader theme that cardiovascular risk should probably be part of the conversation when we’re telling people how to move and train.
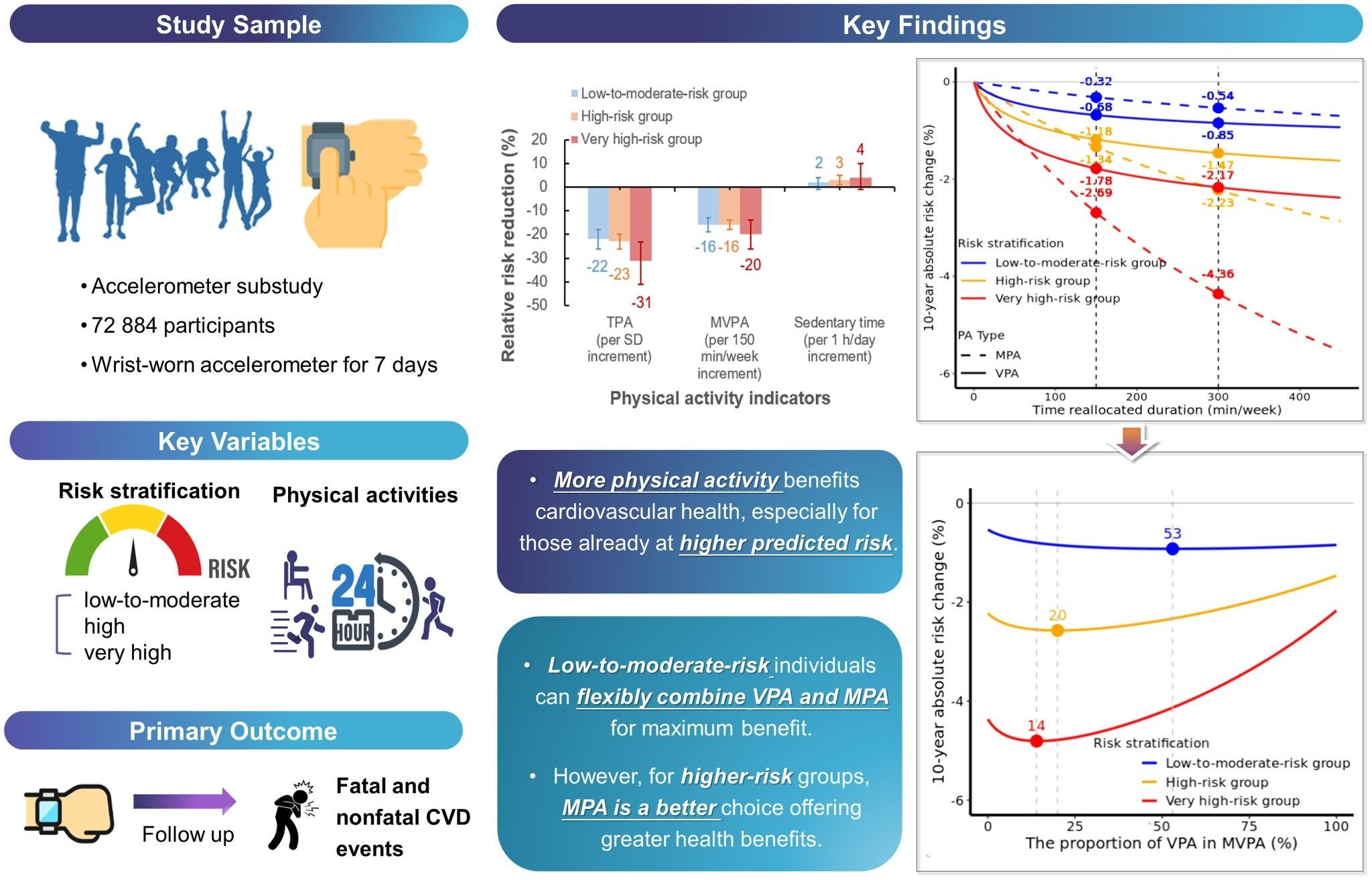
The study drew on data from 72,884 participants in the UK Biobank cohort. At the start, everyone wore an accelerometer (an activity-tracking device) for 7 days, giving researchers an objective look at how much moderate-to-vigorous, moderate-intensity, and vigorous-intensity physical activity people did, along with their sleep and sedentary time.
Researchers then followed participants for about 13 years, tracking cardiovascular disease events including heart disease, stroke, and cardiovascular-related mortality. But instead of simply comparing event rates across different activity levels (which has been done plenty of times before), the novelty was how they framed risk. Participants were first grouped based on how “at risk” they were for cardiovascular disease, using factors like age, total cholesterol and HDL cholesterol, blood pressure, and smoking status; as well as whether they had kidney disease, diabetes, or a family history of high cholesterol. From there, they were classified as low-to-moderate risk, high risk, or very high risk.
With those risk categories in place, physical activity was brought in to answer the study’s central question: “What are the optimal physical activity patterns to promote cardiovascular health among people with different levels of cardiovascular disease risk?”
More activity means lower risk (but it’s complicated)
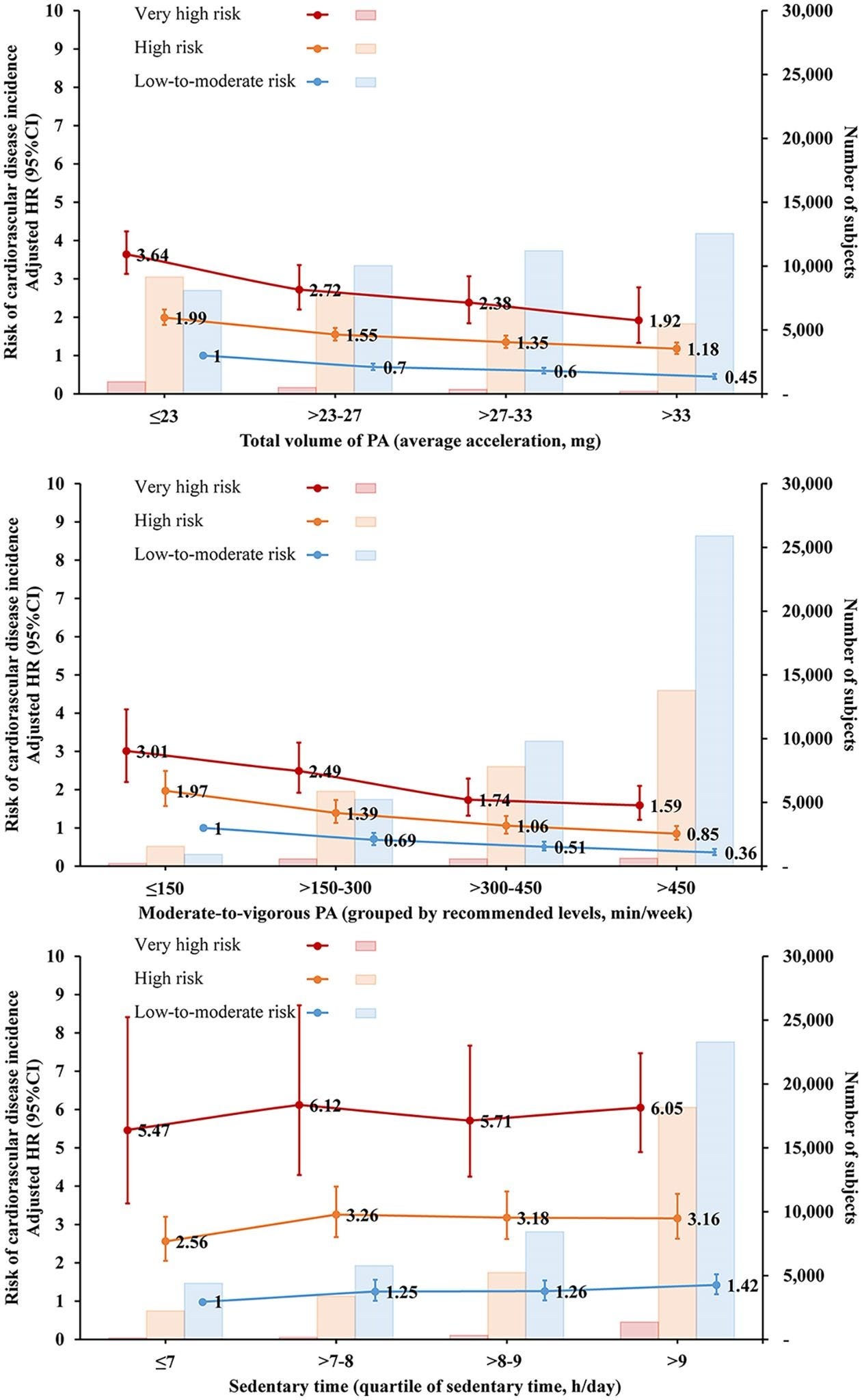
Some of the initial findings were straightforward. Overall, higher levels of physical activity were associated with lower rates of cardiovascular disease across all risk groups in a dose-response manner.
Compared to people who got less than 150 minutes per week, those who achieved 150–300 minutes, 300–450 minutes, and >450 minutes per week had a 28%, 46%, and 58% lower risk of cardiovascular disease (more was better with no apparent upper limit). On the flip side, being sedentary for 7 or more hours per day was associated with a 23–28% greater cardiovascular disease risk (again, no surprise there).
Where things get more interesting is when you layer those relationships onto someone’s baseline risk. In the very high-risk group, additional activity appeared to “matter more” than it did in the low-to-moderate or high-risk groups. For very high-risk individuals, increasing weekly activity by 150 minutes per week was associated with a 20% reduction in cardiovascular disease risk—compared to “just” a 16% reduction for the lower-risk groups.
More moderate activity benefits high-risk groups
At this point, it would be easy to assume the takeaway is simply that more moderate-to-vigorous activity (and especially more vigorous activity) is always better, regardless of risk status. But that’s not exactly what the authors observed.
Instead, the benefits of increasing physical activity differed depending on where someone fell along the cardiovascular risk spectrum.
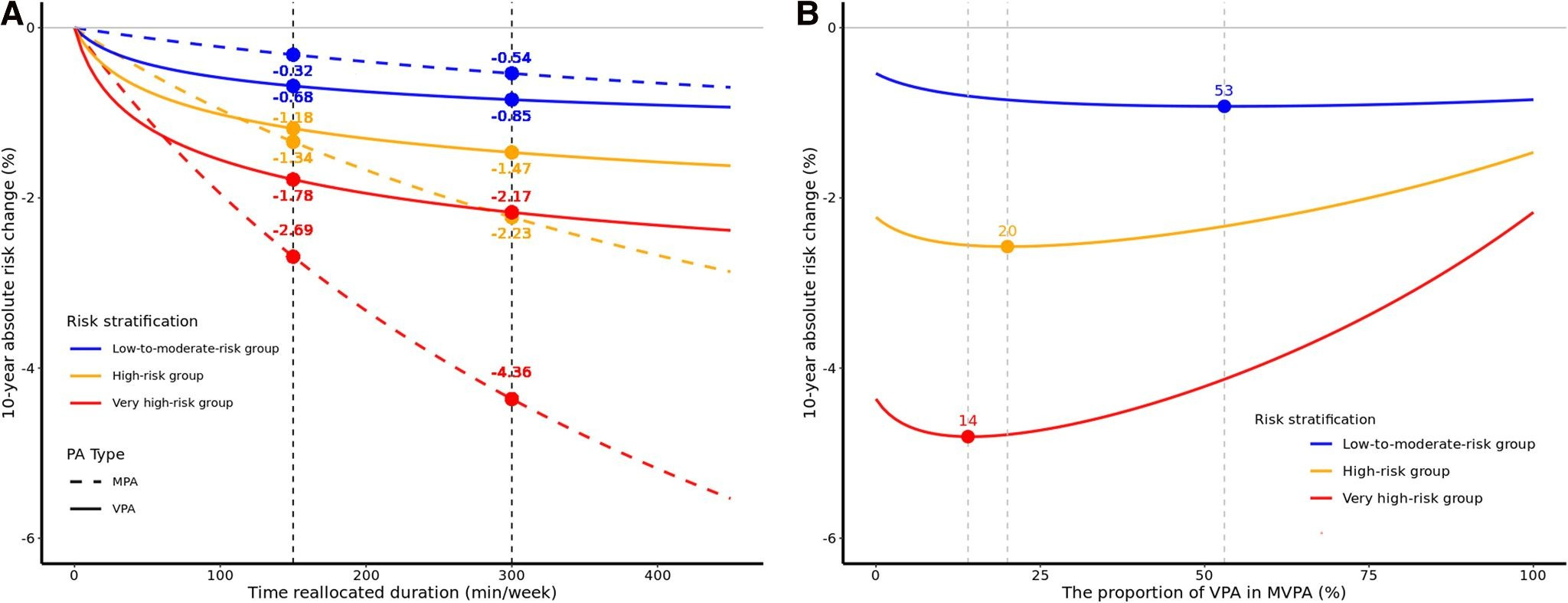
The authors walk through an example of someone “reallocating” 300 minutes of sedentary time to 300 minutes of moderate- or vigorous-intensity activity.
For someone at low-to-moderate cardiovascular disease risk, shifting 300 minutes toward moderate or vigorous activity (and away from sedentary time) reduced their 10-year risk of cardiovascular disease by 0.55% (moderate-intensity) and 0.85% (vigorous-intensity). That’s a small risk reduction, but remember these were already low-risk individuals.
In the high-risk group, the pattern flipped. Replacing sedentary time with 300 minutes of moderate-intensity activity reduced 10-year risk by 2.23%, while replacing it with vigorous activity reduced risk by only 1.47% (i.e., less than moderate-intensity activity). In the very high-risk group, the 10-year risk reduction from 300 minutes more of moderate activity was 4.36%, and for vigorous activity, it was 2.17%.
In short, the benefits of adding more vigorous-intensity activity were less pronounced than adding more moderate-intensity activity for individuals at higher cardiovascular disease risk, suggesting higher-risk individuals may benefit more from swapping sedentary time with moderate activity instead of vigorous (after a certain point, as we’ll see). For low-risk individuals, though, vigorous activity yielded a slightly greater risk reduction compared to the same duration of moderate activity.
The ideal “activity distribution”
The same general theme showed up when the researchers looked at the optimal mix of moderate and vigorous activity.
For low-to-moderate risk individuals, there didn’t seem to be an upper threshold for vigorous activity—spending a higher proportion of weekly activity time at vigorous intensity continued to yield additional benefits.
For high-risk individuals, however, risk reduction peaked when vigorous activity made up about 20% of their total weekly physical activity (about 60 minutes per week for someone engaging in 300 minutes per week). And for very high-risk individuals, the peak occurred when vigorous activity comprised about 14% of weekly physical activity (about 42 minutes per week). Beyond those points, the benefits of adding more vigorous activity started to decline. To be clear, risk never went up (above 0), but the benefits began to plateau or reverse when higher-risk individuals started adding more vigorous activity to their week. Moderate activity, on the other hand, appeared to have no plateau in terms of its benefits when replacing weekly sedentary time.
Whenever there’s a “surprising” finding—even (or perhaps especially) in observational research like the study we’ve been discussing—my first instinct is to ask: why? I think it helps to bring some applicability to what otherwise is just an association.
Why would someone at higher cardiovascular risk not derive the same (or even greater) benefit from adding more vigorous or high-intensity activity as someone at lower risk? On the surface, it feels counterintuitive.
To their credit, the authors did offer some speculation. They suggest that in high-risk individuals—who often already have elevated blood pressure and chronic inflammation—the more intense physiological stress of vigorous activity (on blood pressure, inflammatory molecules, and even hemodynamic stress within blood vessels) could potentially blunt some of its added benefits.
That could be true. But given the broader body of evidence, including randomized controlled trials showing benefits of high-intensity activity in people with preexisting conditions, I’m not fully sold that this is the main explanation.
Instead, I think this result may be less about vigorous activity having limited benefits per se and more about tradeoffs.
Because the substitution model the authors used holds total moderate-to-vigorous activity constant, meaning that “more vigorous” automatically means “less moderate.” And for higher-risk individuals, vigorous minutes may not represent the same physiological dose in the first place. What gets labeled as “vigorous” by an accelerometer could feel much closer to all-out effort for someone who’s less fit or has more comorbidities. Put those two together, and it’s easy to see how, beyond a certain point, swapping moderate minutes for vigorous minutes might stop adding extra protection.
There’s another, simpler possibility that moderate activity may already be doing so much heavy lifting in higher-risk people that the marginal gains from stepping up to vigorous intensity just aren’t as dramatic. When baseline risk is high, any consistent movement can substantially move the needle, so the jump from moderate to vigorous may look smaller than we’d expect.
Whatever the mechanism, one thing feels clear, and it has very little to do with the hazard ratios and modeling details that dominate papers like this.
Personalized activity guidelines are a no-brainer.
The idea that everyone benefits equally from 150–300 minutes of activity per week (or that 75–100 minutes of it should be intense) is insultingly simple. If your goal is reducing cardiovascular disease risk, you should likely move differently than someone whose primary goal is weight loss. And as this study highlights, baseline cardiovascular risk probably deserves a seat at the table when we think about how to distribute intensity across the week.
What’s somewhat serendipitous is that this study echoes a pattern we’ve seen for decades in endurance athletes—the “80/20” approach, where roughly ~80% of training is lower intensity and ~20% is higher-intensity work. In this study, the plateau for vigorous activity among high-risk individuals appeared right around that same 20% threshold.
Does that mean you should train like an athlete if your goal is to maximally reduce cardiovascular disease risk?
It might not hurt.
Thanks for reading. See you next Friday.
~Brady~
Ketone-IQ is high-performance energy in a bottle. I use it for post-exercise recovery along with enhancing focus, mood, and cognition. Take 30% off your order.

Create is the first “modern creatine” brand. They sell a wide range of creatine monohydrate gummies—and yeah, their gummies actually contain creatine, unlike some other brands. They’re giving my audience 20% off their order.

ProBio Nutrition—the all-in-one supplement that I use every single day—is offering 20% off. My preference is the tangy orange flavor, but they also sell an unflavored “smoothie booster” that’s great in a shake, smoothie, or juice.

Equip Foods makes some of the cleanest, best-tasting protein products around. I am absolutely obsessed with their Prime grass-fed protein bars (the peanut butter ones are to die for). Take 35% off a subscription.

Great fun reading about a study that i was a part of. I have given UK Biobank access to my body & soul for about 30yrs. And they get my brain when I am dead too.
My observation about running advice that's out there on line, is that it all seems to be written as if everyone is around 30 to 45 years old. So I have to reinterpret it for myself at 68. For anyone 50 and up who wants to start exercising I'd urge them to get a phys. exam. from a PCP first.