
Red Meat and Diabetes: Untangling Causation from Correlation
Should you skip the steak in hopes of improving your health?


Greetings.
In this week's post, we take a deep dive into the latest study showing that red meat intake is associated with type 2 diabetes…one that caused quite a stir in the media. Whether you’re plant-based or full-on-carnivore, you’ll be interested in what this study does (and doesn’t) say about dietary intake and disease risk.
More meat, more diabetes?
It seems as though every published paper in the field of nutrition science leaves waves of controversy and disagreement as it crashes its way through our news feeds. A new paper published earlier this month in the American Journal of Clinical Nutrition was no exception.1
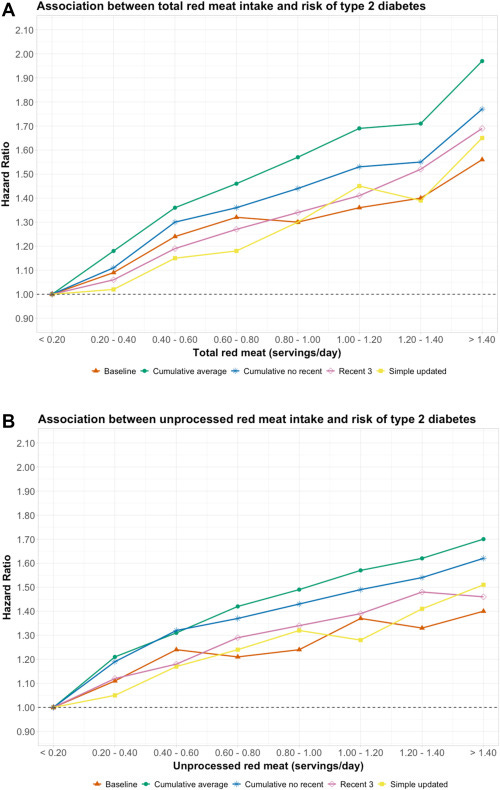
The polarizing study investigated the association between red meat and type 2 diabetes mellitus (T2DM) incidence in three American prospective cohorts: the Nurses' Health Studies I, (NHS-I), Nurses' Health Studies II (NHS-II), and the Health Professionals Follow-up Study (HPFS). The results were consistent with much of the epidemiological evidence we have on the research question, showing a statistically significant increase in the risk of T2DM with higher red meat intake among all three cohorts.

As you might imagine, these findings stirred an enormous amount of heated debate and discussion. The results were naturally applauded by anti-meat and plant-based diet advocates like vegans, whereas crowds more favorable to red meat, such as the keto or carnivore communities, unsurprisingly criticized the study for its design and epistemic virtues, among other nits to pick.
However, neither group's appraisal of the study is likely to be particularly accurate or rigorous — a lot of emotion gets involved in nutrition.
So, let's dive into the details ourselves.
Over the course of 5,483,981 person-years, the study documented 22,761 cases of T2DM, with the average ages for each cohort being 46.1 in the NHS-I, 36.1 years in the NHS-II, and 53.0 years in the HPFS. The study found that a single serving per day increase in total, unprocessed, and processed red meat resulted in a 1.28, 1.24, and 1.46 times higher hazard ratio for T2DM, respectively — in other words, a 28%, 24%, and 46% greater risk.
Keep in mind that the authors defined serving sizes using FDA standards, with a serving of unprocessed red meat being 85g (beef, pork, or lamb) and a serving of processed meat being 28g of bacon or 45g of deli meats.

Compared to those in the lowest quintile of intake, those in the highest quintile for total, unprocessed, and processed red meat consumption had an elevated risk of 62%, 40%, and 51%, respectively. However, after adjusting for variables like body mass index (BMI), which could be a mediator, the associations became substantially weaker, suggesting BMI plays a major role in this relationship.
Furthermore, the analysis indicated that more than half of the relationship between red meat intake and T2DM risk could be statistically accounted for by changes in BMI over time. When the analysis was adjusted to consider both processed and unprocessed red meats simultaneously, the links with T2DM lessened even more, but remained statistically significant. Additionally, there was a consistent positive association between all types of red meat and T2DM across various subgroups.
Counterintuitively, those with higher physical activity levels showed a higher risk of T2DM associated with red meat consumption. The association was also more pronounced among past smokers than current smokers. These results would be perplexing to explain for anyone looking to dismiss the results on the basis of the "healthy user bias", as it appears that certain healthier behaviors seemed to be more strongly associated with a greater risk, not a lesser one.
In the authors' analysis, they cleverly included three different adjustment models that really clearly illustrate just how far nutritional epidemiology has come as a science.
In model 1, we see a basic adjustment model that stratifies participants based on their age, while also accounting for total energy intake. Model 2 builds on model 1 by introducing a more comprehensive set of adjustments, such as race/ethnicity, smoking status, alcohol consumption, physical activity levels, multivitamin use, menopausal status and hormone use, family history of certain diseases, medication use, a litany of dietary components, socioeconomic status, and lastly — and also most importantly — BMI. This is where the authors make a very critical move. Model 3 is nearly identical to model 2, but omits the adjustment for BMI.
You can think of model 2 as accounting for the effect of BMI and thus revealing the BMI-independent effects of red meat itself, whereas model 3 does not account for BMI and allows the variable to influence the results. Per single serving of total, unprocessed, and processed red meat intake, adjusting for BMI reduced the hazard ratios from 1.28 to 1.12, 1.24 to 1.10, and 1.46 to 1.21, respectively.
Now, don't let these massive risk reductions and smaller resulting numbers fool you. The incidence rate of T2DM was over 10% in this study, which means that even a hazard ratio of 1.10 for unprocessed red meat, for example, could still be quite concerning. Or maybe not, if we have a good reason to doubt that this association represents a causal relationship to begin with, which could certainly be the case.
Could red meat intake be causing diabetes?
