
Physiology Friday #179: Is ‘Long COVID’ a Disease of Mitochondrial Dysfunction?
Prevailing coronavirus symptoms may be explained by the virus’s effects on our cellular powerhouses.

Greetings!
Welcome to the Physiology Friday newsletter.
This newsletter is brought to you by Examine.com, PodScholars, and my new eBook, “VO2 Max Essentials”, details for which can be found at the end of this newsletter.
Most of us would like to believe that we’ve moved beyond the COVID-19 pandemic — or at least that society is on the tail end of what was certainly a tumultuous 3+ years
While cases of active COVID may not be as prevalent as they once were, we now have to deal with the economic, political, social, and physical reverberations of the virus. Regarding the latter, post-COVID physical disability may be a “second-wave” of the pandemic that we are inadequately prepared to handle.
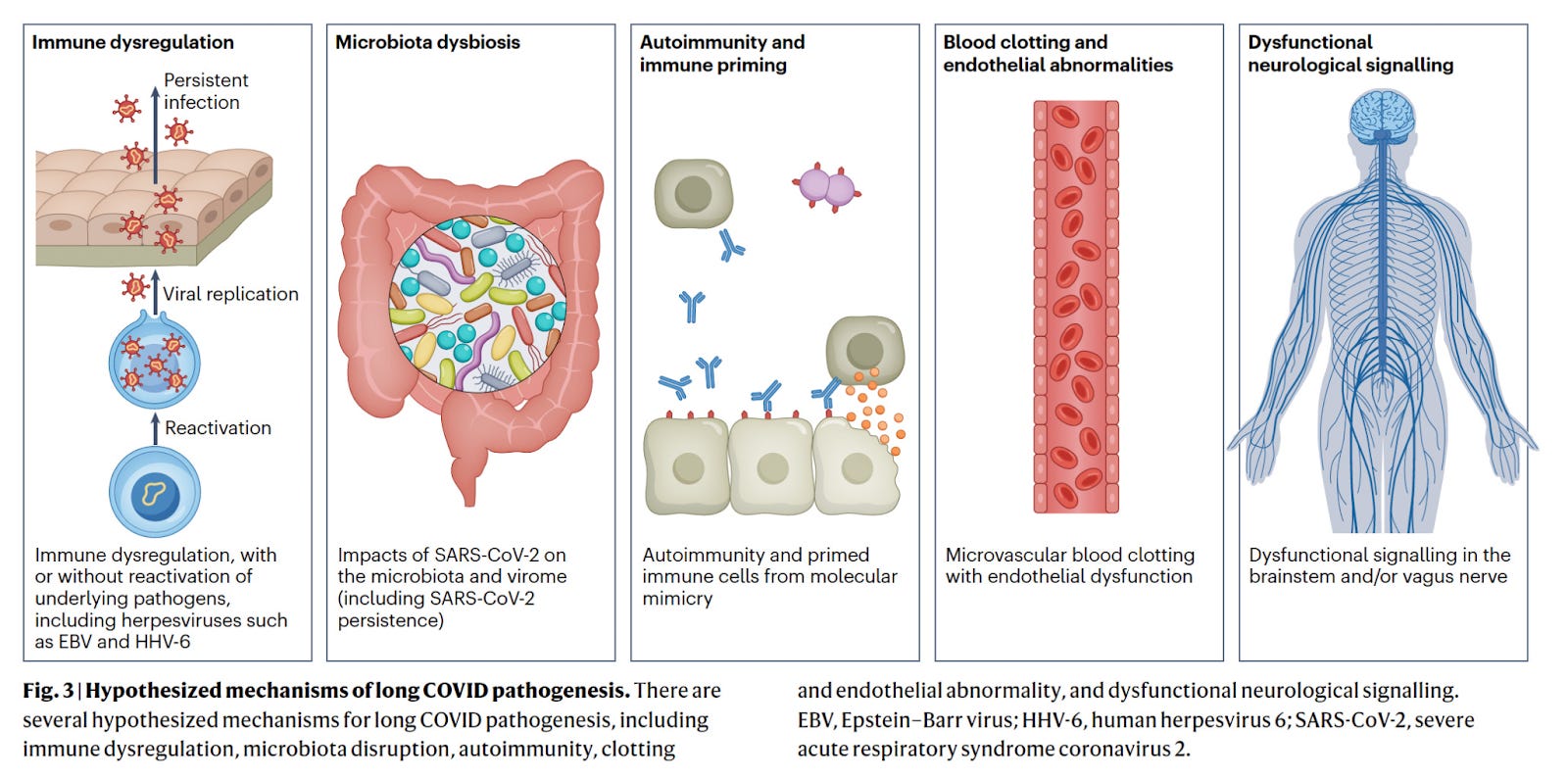
"Long COVID", also known as "post-acute sequelae of SARS-CoV-2 infection", refers to a condition characterized by persistent and often diverse symptoms that continue for weeks to months after the acute phase of COVID-19 has resolved. Long COVID may affect over 10% of cases and manifests with more than 200 symptoms — fatigue, shortness of breath, cognitive impairment ("brain fog"), joint pain, and others — which can affect multiple organ systems, including but not limited to respiratory, cardiovascular, neurological, and musculoskeletal systems.1
The underlying mechanisms for these persistent symptoms are still being studied, but they may involve a combination of viral effects, immune dysregulation, and other physiological disruptions.
Long COVID has been observed in individuals who experienced both mild and severe initial COVID-19 infections, and its prevalence and impact underscore the need for ongoing research to better understand its causes, mechanisms, risk factors, and effective management strategies.
However, original hypotheses into what mechanisms might explain long COVID may have omitted one especially crucial area of physiology — our mitochondria.
How our mitochondria function
I promise not to bore your with a biochemistry lesson, but let’s briefly tackle some basics of how our mitochondria (our body’s “energy powerhouses”) do their job.
Under normal conditions, our mitochondria use energetic substrates — derived from carbon from the food we’ve eaten and digested — to produce energy in the form of ATP in a process known as oxidative phosphorylation (OXPHOS).
During OXPHYS, NADH and FADH2 (produced during another process known as the Krebs or TCA cycle) are shuttled about through a multi-protein complex known as the electron transport chain, which pumps protons (H+ molecules) to generate a membrane potential. This chemical energy is then used to convert a molecule called adenosine diphosphate (ADP) into ATP (energy!)2

In contrast, dysfunctional mitochondria are characterized by high levels of reactive oxygen species, calcium overload, an opening of the mitochondrial permeability transition pore, and the induction of cell death (apoptosis). These culminate in the loss of the mitochondrial membrane potential and a reduction in the energy-generating potential of the mitochondria. Not a good place to be in.
As it turns out, SARS-CoV-2 viral proteins can bind to mitochondrial proteins in the hosts they infect, and in a recent study published in the journal Science,3 researchers uncovered how COVID-19 may influence mitochondrial function, with implications for the symptoms observed in long COVID sufferers and potential treatments for those afflicted.
In the study, researchers analyzed mitochondrial gene expression in nasopharyngeal samples from humans who had been infected with COVID-19, as well as autopsy tissues from patients who had COVID-19 at the time of death.
In the nasopharyngeal samples, the virus was found to block transcription of nuclear DNA-encoded mitochondrial OXPHOS genes and activate a protein known as hypoxia-inducible factor-1 alpha (HIF-1ɑ) to induce glycolysis (a process by which our body produces energy by breaking down glucose). In addition, the virus activated immune defenses and initiated stress responses.

In the autopsy tissues, even though COVID-19 was no longer present, nuclear DNA mitochondrial gene expression was impaired in the heart, kidney, and liver, while immune defense pathways and mitochondrial DNA gene expression were upregulated. Interestingly, mitochondrial gene transcription in the lungs had recovered.
Further studies were conducted in hamsters, in whom it was found that in the early phase of COVID-19 when viral load was at its peak, mitochondrial gene expression in the lungs was somewhat preserved, while that in certain areas of the brain was suppressed — despite the absence of the virus in these areas. Later on — when viral load began to decline — gene expression recovered in the lungs.
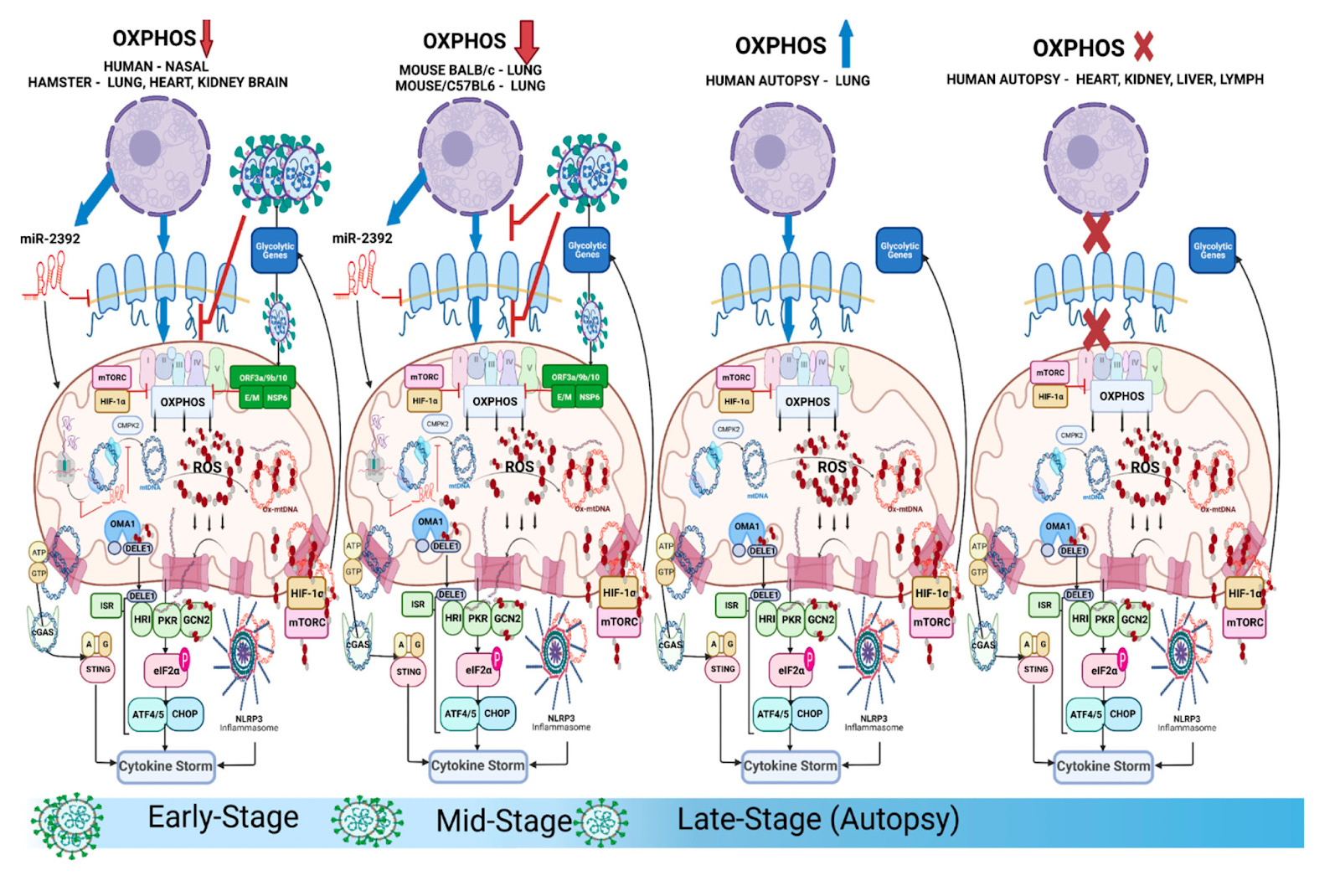
The findings support the idea of persistent heart, kidney, and liver dysfunction, among others, in the pathology of long COVID. The lungs — the first “target” of SARS-CoV-2 — seem to be the first organ to recover, while other vital organs remain impaired even after the viral load had declined or diminished altogether.
These effects seem to be due to the virus “hijacking” mitochondria and the host cell’s attempt to compensate by activating innate immune defenses and even upregulating the production of mitochondria/mitochondrial proteins — which ultimately prove to be futile.

If you are or have known someone that’s been affected or is still affected with long COVID symptoms, these findings may not be surprising. Many complain of a poor exercise capacity, lingering brain fog, shortness of breath, and an impaired ability to engage in activities they once found easy. In other words, things that require functional mitochondria.
We have a LOT to understand about long COVID, how it affects the body, how long it lasts, and what really causes it. However, this study identifies the mitochondria as a “novel” contributor to long COVID, and I think the implications for treatment are apparent.
Pharmacological therapies and nutraceuticals (i.e., rapamycin, metformin, mitochondrial-targeted antioxidants) to restore mitochondrial OXPHOS capacity may prove useful.
But the glaringly obvious solution must involve exercise.
At this point, it’s too late to talk about how better metabolic fitness could have helped to prevent or at least lessen the burden of COVID-19 in many people. We know that poor metabolic health and aerobic fitness are risk factors for COVID-19 morbidity and mortality.
The inactivity that resulted from COVID-19-related precautionary measures probably wasn’t great for population-wide health, especially in light of these findings. this has nothing to say about the effectiveness of those interventions in the management of the pandemic. However, we can recognize the role that exercise therapy could play in the rehabilitation of people with long COVID and design well-controlled research studies to examine its effects on disease regression and symptom curtailment.
I’m not going to say that exercise is or could have been a panacea to the pandemic, but it wouldn’t have hurt, and it certainly won’t hurt to promote more exercise going forward. We owe it to our mitochondria.
Thanks for reading. See you next Friday.
~Brady~

The VO2 Max Essentials eBook is your comprehensive guide to aerobic fitness, how to improve it, and its importance for health, performance, and longevity. Get your copy today and use code SUBSTACK20 at checkout for a 20% discount.

Examine.com: Examine is the largest database of nutrition and supplement information on the internet.

PodScholars: PodScholars is the first podcasting platform and database specifically geared towards published research, where scholars, researchers, and other experts can broadcast published science as audio or video casts.
The question is if the virus induced apoptosis and you haven’t been infected for a while, how are the mitochondrial effects persisting? At a certain point you should clear the infection, and unless there is a DNA modification in viable human cells which persists and is producing more of the offending proteins which then creates a chronic condition. Some people are recommending nattokinase for treatment of long COVID, but I’ve yet to see any data in efficacy or its mechanism in this context.