
Physiology Friday #214: Strengthening the Link Between V̇O2 Max and Longevity & Healthspan
Get fitter. Live longer.

Greetings!
Welcome to the Physiology Friday newsletter.
ICYMI
Check out my guest appearance on The Neuro Experience podcast with Louisa Nicola, where we talk about the science of V̇O2 max.
On Wednesday, I published a post about some of the most common myths about coffee and caffeine.
Details about the sponsors of this newsletter including Examine.com and my book “VO2 Max Essentials” can be found at the end of the post!
If you can fill the unforgiving minute
With sixty seconds’ worth of distance run,
Yours is the Earth and everything that’s in it,
And—which is more—you’ll be a Man, my son!
— Rudyard Kipling, If—
In my book “VO2 Max Essentials”, I make the case for why cardiorespiratory fitness should be considered the most important vital sign. Among all risk factors, V̇O2 max is the only one that’s a composite of multiple physiological systems, rather than a snapshot of health at one point in time or a single biomarker measured via a blood test.
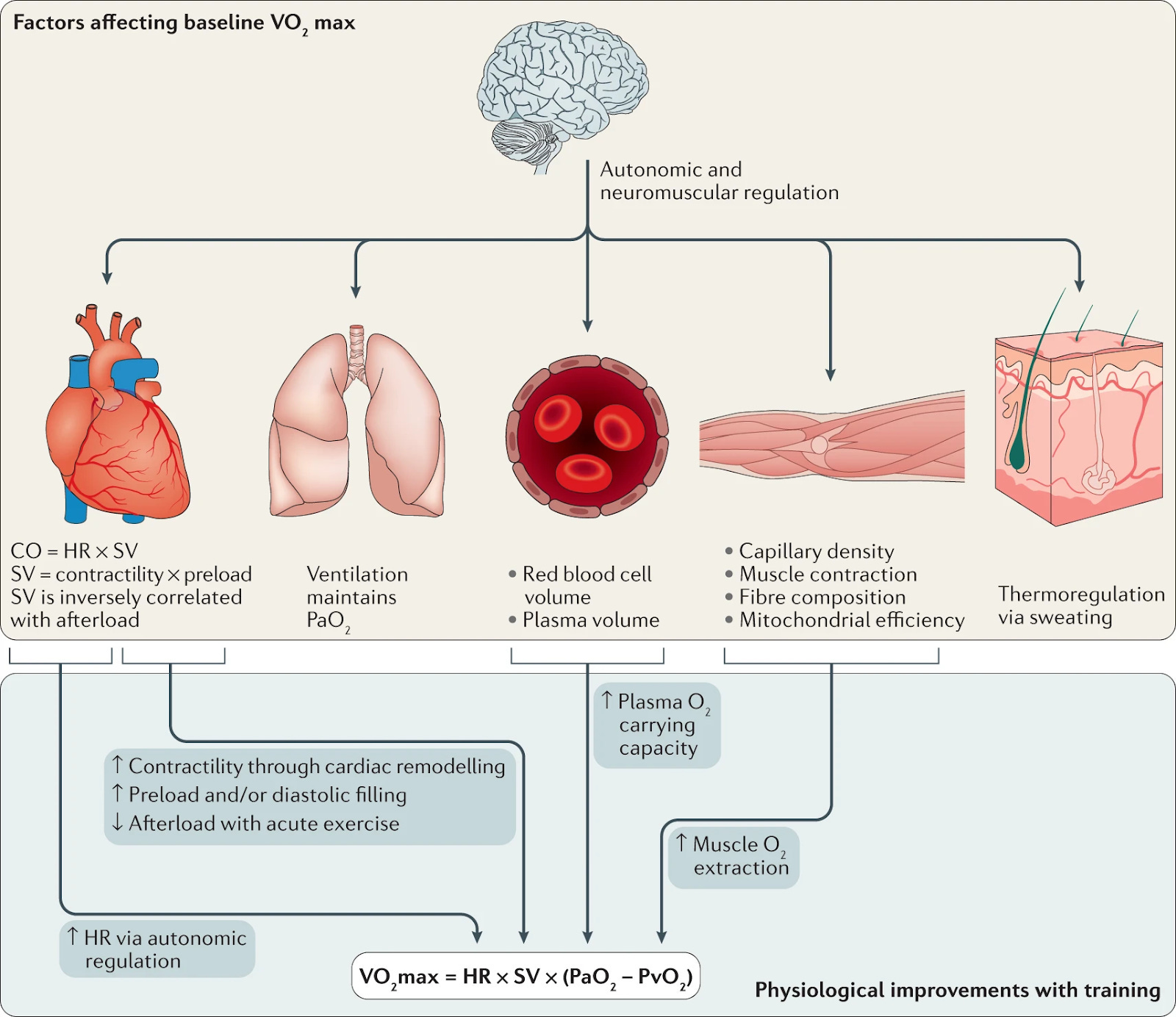
Your maximal oxygen utilization capacity (V̇O2 max) represents the maximum integrated capacity of the pulmonary, cardiovascular, and muscular systems to uptake, transport, and utilize oxygen during whole-body, dynamic exercise. The function of your autonomic nervous system, your heart and blood vessels, your lungs, your muscles, and your mitochondria all influence your maximal aerobic capacity. It’s not just a strong heart that gives someone a high V̇O2 max. A strong body is a prerequisite.
This is, in my opinion, why a high V̇O2 max is so often associated with beneficial health outcomes. You won’t find someone with a high V̇O2 max who is in poor health, and often people with an extremely low V̇O2 max are in poor health.
Though it’s not routinely measured in clinical practice (yet), V̇O2 max has recently appeared on the radar of many healthcare professionals. People are becoming aware of the predictive power of cardiorespiratory fitness and are increasingly interested in how (and why) to improve it.
Over the last 20 years, evidence has emerged linking higher cardiorespiratory fitness to lower risks of all-cause mortality and other diseases. Thus, it’s about time we had a scoping review of the evidence, which brings us to today’s study.
The study, published in the British Journal of Sports Medicine1 was an overview of all previously published systematic reviews and meta-analyses on the relationship between V̇O2 max and an array of health outcomes.
The studies were eligible if they included adults with or without health conditions and measured cardiorespiratory fitness using a maximal graded exercise test, a maximal or submaximal exercise test with a prediction equation (i.e., without direct measures of gas exchange), or a non-exercise prediction equation. When pooling the data and examining the outcomes, the authors compared the groups with the highest cardiorespiratory fitness to those with the lowest cardiorespiratory fitness.
Overall, a total of 26 studies with over 20.9 million participants from 199 different cohorts were included in the review.
Eight of the included studies examined the association between V̇O2 max and death (mortality) from all causes, cardiovascular disease, sudden cardiac events, all cancers, and lung cancer.
Compared to low cardiorespiratory fitness, having high cardiorespiratory fitness was associated with a 41% to 53% lower risk for premature mortality. Furthermore, each 1 metabolic equivalent (MET) increase in cardiorespiratory fitness (1 MET is equal to an increase in V̇O2 max of 3.5 mL/kg/min) reduced the risk of premature mortality by 7% (all cancers) to 51% (sudden cardiac mortality).
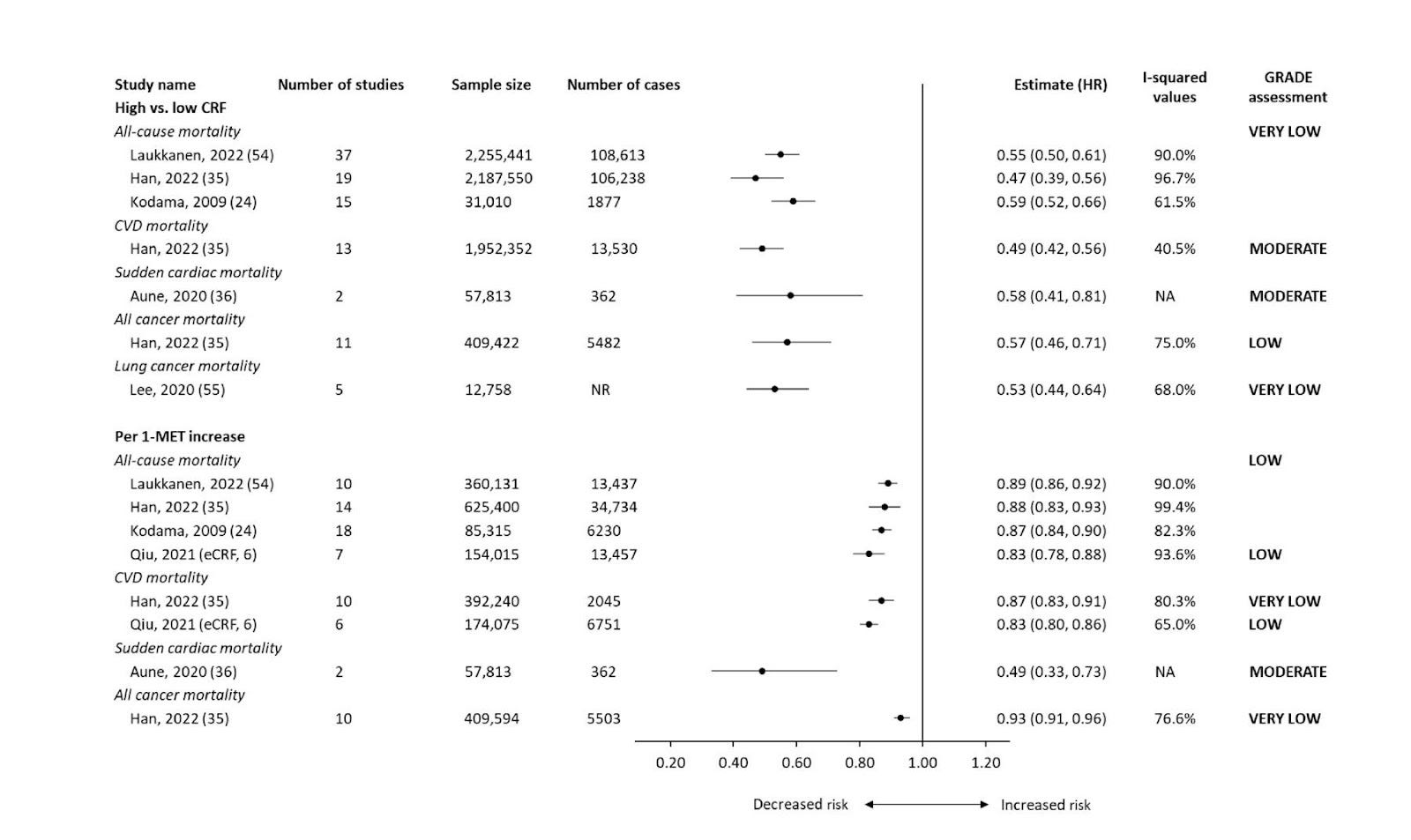
A notable limitation for mortality outcomes was the large disparity in male vs. female participants — more than 1.8 million male participants were included in the studies while only 180,000 females were included.
Having a higher cardiorespiratory fitness was also associated with a lower risk of developing hypertension, heart failure, stroke, atrial fibrillation dementia, kidney disease, depression, and type 2 diabetes. Specifically, the risk of a new onset condition was 37% (hypertension) to 69% (heart failure) lower when comparing high vs. low cardiorespiratory fitness.
For every 1 MET increase in fitness, the risk of developing a new chronic health condition was reduced by 3% (stroke) to 18% (heart failure).
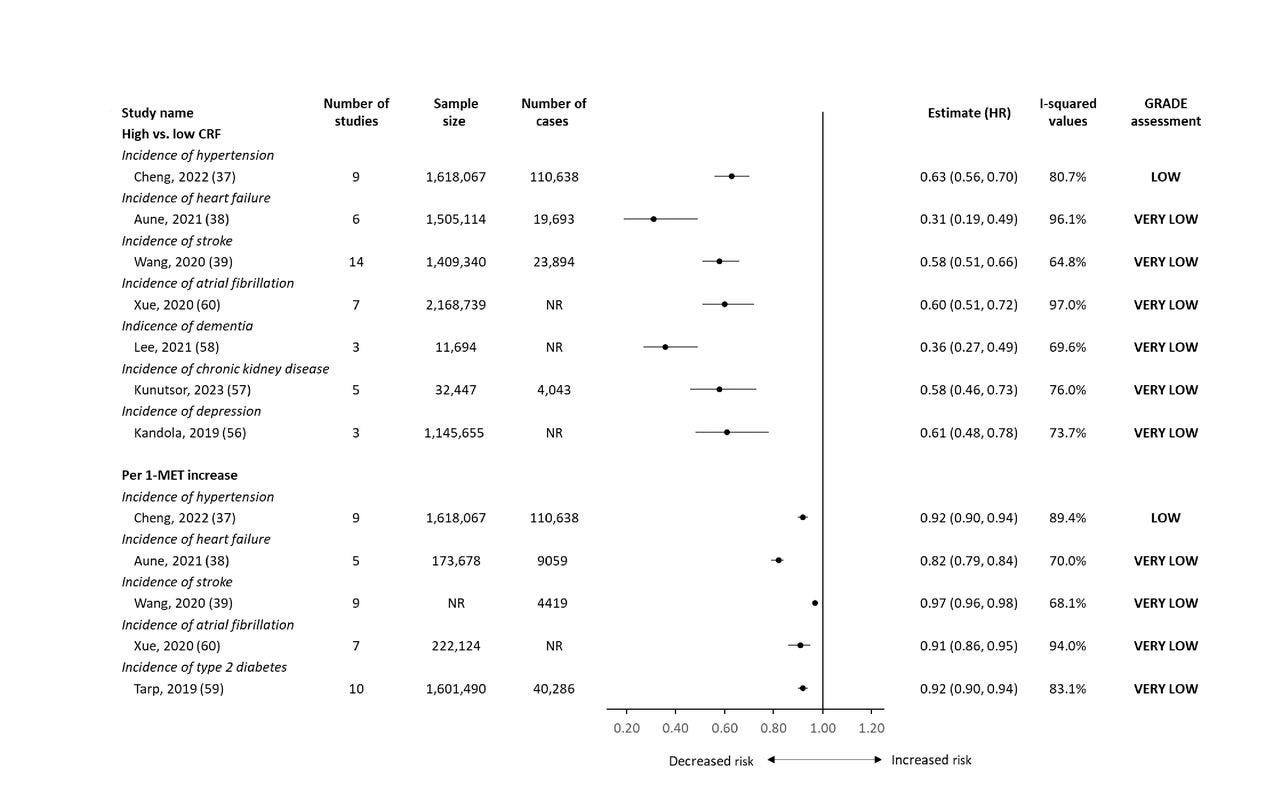
Similar to mortality outcomes, a majority of the evidence was from male populations, although two studies investigated the effects in female-only cohorts. In these groups, high cardiorespiratory fitness was found to be more protective against stroke and type 2 diabetes among females compared to males. Among men, a higher cardiorespiratory fitness was not associated with prostate cancer risk.
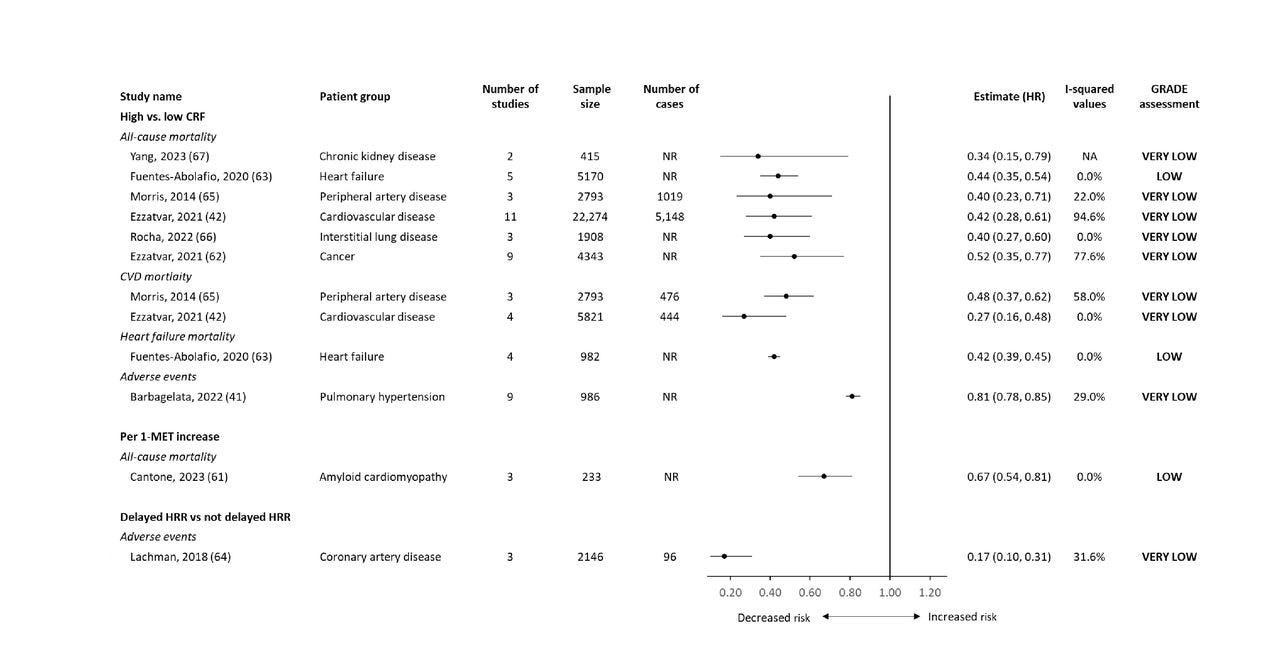
What about individuals who already have a chronic health condition? Does having a high cardiorespiratory fitness protect them from early death or adverse events?
This seems to be the case. A lower risk of premature death or adverse events was observed for people with a higher vs. a lower cardiorespiratory fitness and ranged from 19% (for an adverse event among adults with pulmonary hypertension) to 73% (for cardiovascular mortality among people living with cardiovascular disease).
Based on this comprehensive review, not only does having a higher cardiorespiratory fitness reduce the risk of premature death from all causes, but it also reduces the risk of developing a new condition or dying from a condition you already have.
Put another way, low fitness is a consistent and important risk factor for early death and chronic disease.
If this isn’t enough evidence that cardiorespiratory fitness should be considered a vital sign, I don’t know what is. The authors even suggest that a minimum clinically important difference or MCID for V̇O2 max be established as 1 MET (3.5 mL/kg/min). Exercise trials and other interventions can be deemed “effective” if the participants achieve this degree of fitness improvement. It’s a goal you should strive for in your own exercise regimen.
Because this was merely an overview of published literature, we unfortunately don’t have specific numbers for the “high” and “low” V̇O2 max groups. But I did a quick scan of the included studies on mortality risk to find a quick estimate.
Low cardiorespiratory fitness is somewhere in the range of less than 8—9.5 METs or a V̇O2 max of less than 28—33 mL/kg/min. High cardiorespiratory fitness is about 11—13.7 METs or more, or a V̇O2 max of 38.5—48. If you’re below or near one of these categories, act accordingly.
The certainty (quality) of the evidence was also downgraded mostly due to a large variation in how the studies measured V̇O2 max and the large proportion of male participants. And, of course, the main limitation is that these associations (correlations) may not imply causation.
One of the main criticisms of this literature is that, because nearly 50% of one’s V̇O2 max can be explained by genetics and is therefore unmodifiable, the association between cardiorespiratory fitness and healthspan/longevity may not represent an effect of a high fitness level per se, but rather, an underlying predisposition to health. Healthy people have a higher V̇O2 max, but they’re not healthy because of it.
I don’t buy this. To explain why, I’ll use the Bradford Hill criteria.
The Bradford Hill criteria, also known as Hill’s criteria for causation, are a set of nine principles used to establish epidemiologic evidence of a causal relationship between a presumed cause and an observed effect. These criteria have been widely used in public health research and were proposed by the English epidemiologist Sir Austin Bradford Hill in 1965.
The nine criteria are:
Strength (Effect Size)
A small association does not rule out causality, but a stronger association increases the likelihood of a causal effect.
Consistency (Reproducibility)
Consistent findings across different studies, populations, and settings strengthen the evidence for causality.
Specificity
A specific association between a factor and an effect suggests a higher probability of a causal relationship.
Temporality
The cause must precede the effect in time
Biological Gradient (Dose-Response Relationship)
Generally, greater exposure leads to a higher incidence of the effect.
Plausibility
A plausible mechanism linking cause and effect enhances the evidence.
Coherence
Consistency between epidemiological findings and laboratory evidence strengthens the likelihood of causality.
Experiment
Experimental evidence can support causality.
Analogy
Similarities between the observed association and other known causal relationships can provide additional support.
Now, let’s apply the Bradford Hill criteria to V̇O2 max.
Strength of Association
Numerous studies consistently demonstrate a strong inverse relationship between cardiorespiratory fitness and mortality risk. Case in point: this review.
Consistency of Effect
Research findings consistently support the link between fitness and health outcomes. Multiple studies across diverse populations consistently show that better fitness is associated with improved health and longevity. Again: see this review.
Specificity
While cardiorespiratory fitness impacts overall health, it specifically reduces the risk of cardiovascular diseases, diabetes, and certain cancers.
Temporality
The temporal relationship is well-established: higher fitness precedes better health outcomes. Individuals who maintain or improve their fitness levels over time experience reduced mortality risk.
Dose-Response Relationship
A dose-response pattern exists: as cardiorespiratory fitness increases, mortality risk decreases.
Plausibility
Mechanisms underlying this association include improved cardiovascular function, enhanced metabolic health, and reduced inflammation. We know that regular exercise improves heart health, insulin sensitivity, lipid profiles, and overall physiological function.
Coherence
The association aligns with existing knowledge about exercise physiology and health.
Experiment
Although we cannot perform a randomized controlled trial where we randomly assign people to have higher VO2 max, observational studies provide strong evidence.
Analogy
Analogously, we can draw from other well-established causal relationships. For example, the association between smoking and lung cancer was initially based on observational studies, and later experimental evidence confirmed the causal link.
The evidence (and my personal biases) would indicate that improving fitness is a cause of better health. I explain why this may be the case in my book.
If you don’t know your V̇O2 max, I provide several methods to estimate V̇O2 max in my book, and for a limited time, I made this chapter open to everyone on my Substack. Feel free to look at some of the protocols and do some testing!

Regardless of your current fitness level, take comfort in knowing that improving your V̇O2 max by 1–3 METs (and reducing your risk of death and disease substantially) is very attainable with some dedicated aerobic exercise training.
Out of all of the risk factors, V̇O2 max is the one that’s most fun to improve. It might also be the most important.
Thanks for reading. I’ll see you next Friday.
~Brady~

The VO2 Max Essentials eBook is your comprehensive guide to aerobic fitness, how to improve it, and its importance for health, performance, and longevity. Get your copy today and use code SUBSTACK20 at checkout for a 20% discount. You can also grab the Kindle eBook, paperback, or hardcover version on Amazon.

Examine.com: Examine is the largest database of nutrition and supplement information on the internet.
What do you think about the suggestion that it isn’t the vo2 that provides the benefit. Instead it is all the activity that is needed to have a high vo2. If this is true then training specifically to improve vo2 would not be nearly as important as just having high activity levels?
I guess that is my point. It would be nice to see a study that compares outcomes against physical activity vs VO2max. Not sure how you would do that, but if you could find people with lower VO2max but lots of activity and if these people were not equally protected, that would tell you that VO2max is the thing. Probably not enough people out there with high activity and lower VO2max to make things statistically significant? I know I have seen papers that show high activity level is also protective….just not sure if anyone has ever compared activity to VO2max?